- Home
- Dr Shailesh Keshav Mishra
- Arthroscopy
- Joint Replacement surgeries
- Arthritis care
- Type of Sports injuries
- Gallery
- Blogs
- Testimonials
- Contact Us





Joint preservation surgery to repair damage to articular cartilage inflicted by osteoarthritis and malalignment
With each step, forces equal to three to eight times your body weight travel between the thigh bone (femur) and shin bone (tibia) in your knee. These forces are dampened by a meniscus on the inner and outer portion of the knee, and the ends of the bones are protected by articular cartilage.
Patients with a condition known as osteoarthritis , or degenerative arthritis, experience a successive wearing on the menisci and articular cartilage, which may develop tears. These degenerative processes limit the ability of the knee to glide smoothly and can result in popping, catching, locking, clicking and pain.
In a condition called malalignment, unbalanced forces cause excessive pressure on either in the inner (medial) or outer (lateral) portion of the knee. Degenerative arthritis and malalignment can cause the knee’s protective tissues to wear on one side more than the other in a repetitive cycle of damage. A partial or total knee replacement can correct this condition when joint damage is beyond repair.
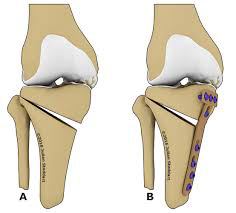
In certain cases, however, a technique known as osteotomy can can realign the knee, taking pressure off the damaged side. A procedure known as a high tibial osteotomy wedges open the upper shin bone (tibia) to reconfigure the knee joint. The weight-bearing part of the knee is shifted from degenerative or worn tissue onto healthier tissue.
A high tibial osteotomy is generally considered a method of prolonging the time before a knee replacement is necessary because the benefits typically fade after eight to ten years. This procedure is typically reserved for younger patients with pain resulting from instability and malalignment. An osteotomy may also be performed in conjunction with other joint preservation procedures in order to allow for cartilage repair tissue to grow without being subjected to excessive pressure.
Since it was first performed successfully in 1958, high tibial osteotomy has made its way as a mainstream operation for degenerative arthritis of the knee. The goal of high tibial osteotomy is to re-position and normalize the weight bearing line, so as to reduce the stress impact on medial and lateral compartments. if the patient fills the younger age category with an active lifestyle, osteotomy must be the procedure of choice to cure angular deformity that goes beyond the mean range of physiological variation. For a young adult, osteoarthritis is considered to be mechanical phenomenon. In malaligned knee the pathologiocal phenomenon of meniscal injury, osteochondrial injury and ligamentous insufficiency, may also get added and they can contribute towards the development of arthritis in the young adult. To determine whether a patient needs osteotomy, the orthopedic must look for any malalignment with arthrosis, instability, need for articular cartilage procedure. Studies have shown that younger patients can qualify for an osteotomy if they are suffering from a secondary degenerative arthritis, a localized medial joint pain and a varus knee.
The surgery is performed on the patient in the supine position using a tourniquet. Throughout the surgery fluoroscopic imaging is used as a guide. Halfwaty between the tibail tubercule and the posteromedial border of the tibia an incision is made. A dissection is then extended down to the Sartorius fascia. Using a periosteal elevator, the MCL is retracted medially, which exposes the tibial cortex. After using osteotomes to open the osteotomy in various stages, a four-holed osteotomy plate (like Puddu plate or Tomofix plate) is placed at the osteotomy site.
Conceptualized, Marketed & Promoted by Jaivam Life LLP | Sitemap | Privacy Policy



